The word Eczema, also known as Dermatitis, is derived from the Greek word ‘Ekzein’ which means ‘to boil’ or ‘bubble’. A common dry skin condition that is characterised by red, inflamed and itchy skin, which can occur all over the body and, depending on its severity, is classed as clear, mild, moderate or severe. Patients affected by the condition will go through periods of flare-ups and remissions, although it is not curable, in the majority of cases it can be controlled. Eczema is not contagious and it is worth reminding patients, especially young children, of this fact. There are many different types of eczema and they include:

Eczema
![]() Atopic Eczema
Atopic Eczema
![]() Allergic Contact Eczema
Allergic Contact Eczema
![]() Irritant Contact Eczema
Irritant Contact Eczema
![]() Seborrhoeic Eczema
Seborrhoeic Eczema
![]() Nummular or Discoid Eczema
Nummular or Discoid Eczema
![]() Dyshidrotic, Vesicular or Pompholyx Eczema
Dyshidrotic, Vesicular or Pompholyx Eczema
![]() Lichen Simplex or Neurodermatitis
Lichen Simplex or Neurodermatitis
![]() Stasis, Varicose or Gravitational Eczema
Stasis, Varicose or Gravitational Eczema
![]() Asteatotic Eczema or Eczema Craquelé
Asteatotic Eczema or Eczema Craquelé
Atopic Eczema is the most common form of eczema and affects males and females equally. It can occur at any age however, it is especially common in children.
It affects 1 in 5 children in the UK with about half of these cases improving by the time they reach 11 and two-thirds by the age of 16, unfortunately, even though it improves, there may be flare-ups later in life. Atopic eczema tends to run in families so a child is more likely to develop eczema if one or both parents have it (37.9% and 50% respectively) compared to a child whose parents don’t have it (27.1%). Although there is a family history the link doesn’t always have to be between parent and child as it can skip a generation. Depending on its severity it can cause intense itching which can lead to sleep disturbances affecting the quality of life of the child, parent and/or carer. Eczema can also occur in adults and in fact affects 1 in 12 in the UK.
The exact cause of Atopic Eczema is unknown however it is likely to be a combination of genetic and environmental factors. The genetic part causes a defective skin barrier which makes the skin more susceptible to triggers such as irritants, pathogens and allergens.
Atopic eczema tends to run in families so a child is more likely to develop eczema if one or both parents have it (37.9% and 50% respectively) compared to a child whose parents don’t have it (27.1%). Although there is a family history the link doesn’t always have to be between parent and child as it can skip a generation.
To understand what happens in eczematous skin we must first look at the stratum corneum or skin barrier and its function in healthy skin. The best way to think of this barrier is as a brick wall which, in healthy skin, keeps pathogens, irritants and allergens out whilst preventing the loss of water and other substances. Within the barrier the individual bricks are the corneocytes (anucleated keratinocytes), and these contain Natural Moisturising Factor (NMF), which acts as a humectant and attracts water into them. This causes them to become swollen and sit tightly against each other. The corneocytes are surrounded by the intercellular lipid lamellae (composed of phospholipids, cholesterol and glucosylceramides), which represent the mortar in this analogy and help to retain water within the corneocytes. The intercellular lipid lamellae and swollen corneocytes collectively produce a smooth and strong semi-permeable barrier. There is some water loss through this semi-permeable barrier, which is normal, and is called Transepidermal Water Loss or TWL.
In eczema the skin barrier is no longer effective as a result of the breakdown of the lipid lamellae and a reduction in the amount of NMF in the corneocytes. The net effect is a reduction of water within the corneocytes, which start to shrink causing gaps to form between them. The breakdown of the lipid lamellae also results in cracks starting to appear in the skin (the mortar is crumbling). We now have a barrier with cracks and gaps which allows irritants, allergens and pathogens in and more water, than the normal transepidermal water loss, to be lost. This causes dryness, inflammation, itching and eczema flare-ups.
To find out more about the skin barrier Click here
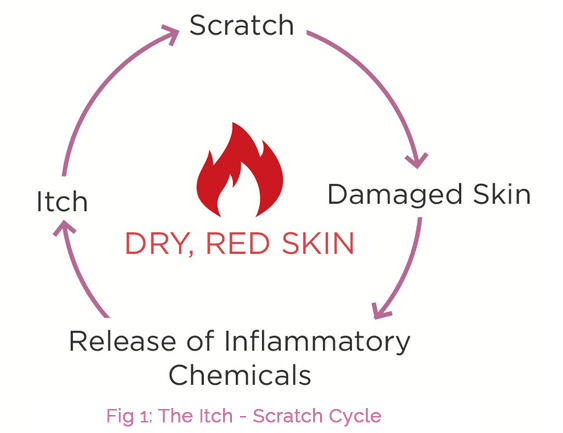
Itching and inflammation can lead to scratching which in turn can lead to further irritation exacerbating the itch-scratch cycle and making the eczema worse. Scratching can also break the skin causing it to bleed, leaving it open to infections and can result in thickening of the skin.
People with eczema have a heightened reaction to sensitisers, irritants, allergens and pathogens so they suffer more inflammation when exposed to them compared to someone who doesn’t have eczema. Certain triggers can cause eczema to flare-up or get worse and not only do these vary from patient to patient but so does a patient’s actual response to them.
Common triggers include:
![]() Sensitisers & irritants in emollients – SLS, parabens, halogens, fragrances and colours.
Sensitisers & irritants in emollients – SLS, parabens, halogens, fragrances and colours.
![]() Irritants – soaps, detergents, bubble baths, washing detergents and disinfectants like chlorine.
Irritants – soaps, detergents, bubble baths, washing detergents and disinfectants like chlorine.
![]() Allergens – pet dander, mould spores and house dust mites.
Allergens – pet dander, mould spores and house dust mites.
![]() Certain fabrics such as wools or dyes and finishes in new clothes.
Certain fabrics such as wools or dyes and finishes in new clothes.
![]() Stress.
Stress.
![]() Microbes – bacteria, fungi and viruses.
Microbes – bacteria, fungi and viruses.
![]() Temperature – extreme hot or cold weather, extremes in humidity – high and low.
Temperature – extreme hot or cold weather, extremes in humidity – high and low.
![]() Foods – examples include nuts and dairy products. Identifying food triggers should only be done with the help of a dietician or doctor.
Foods – examples include nuts and dairy products. Identifying food triggers should only be done with the help of a dietician or doctor.
![]() Pregnancy and hormonal changes before a period.
Pregnancy and hormonal changes before a period.
![]() Sweating during exercise.
Sweating during exercise.
![]() Swimming.
Swimming.
If a patient can identify what triggers their symptoms, they can then avoid them which in turn will reduce the risk of flare-ups, however it can sometimes be difficult to identify triggers and certain triggers, such as pregnancy and hormonal changes before a period, cannot be avoided. Food triggers should only be avoided by a patient after consultation with a healthcare professional such as a dermatologist, doctor or dietician. For more tips and advice to print and give to your patients visit our tips and advice section.
Symptoms of eczema vary depending on the severity of the condition.
In mild cases the skin is:
![]() Dry
Dry
![]() Red
Red
![]() Itchy
Itchy
![]() Scaly
Scaly
Whilst in severe cases it can be:
![]() Intensely and constantly itchy
Intensely and constantly itchy
![]() Inflamed
Inflamed
![]() Weeping
Weeping
![]() Crusted
Crusted
![]() Bleeding
Bleeding
![]() Possibly infected
Possibly infected
![]() There may be darkened or lightened skin patches
There may be darkened or lightened skin patches
Currently there is no cure for eczema, however in the majority of cases the condition can be managed. Patients with eczema all over their body should be reminded that although it may occur all over, each area may differ in severity and so should be treated individually. The first step for a patient in managing the condition would be to avoid any known triggers which, for various reasons, can be difficult in some cases and impossible in others.
Severity of the condition can be classed as:
![]() Clear – skin looks normal and clear.
Clear – skin looks normal and clear.
![]() Mild – in these cases there are some areas of dry skin present, occasional itching and possibly some small parts that are red.
Mild – in these cases there are some areas of dry skin present, occasional itching and possibly some small parts that are red.
![]() Moderate – Areas of dry skin are present, itching occurs often, there are red areas and skin may be damaged, scratched or thickened.
Moderate – Areas of dry skin are present, itching occurs often, there are red areas and skin may be damaged, scratched or thickened.
![]() Severe – There are lots of areas of dry skin, itching is continuous, as well as red areas there may be skin that is damaged or scratched, lots of thickened areas, bleeding, oozing, cracking and changes in skin colour.
Severe – There are lots of areas of dry skin, itching is continuous, as well as red areas there may be skin that is damaged or scratched, lots of thickened areas, bleeding, oozing, cracking and changes in skin colour.
Treatments will vary depending on the severity of the eczema and will be stepped down or up as the condition gets better or worse, however emollients such as AproDerm® form the basis for all treatments and should always be used even when your patients eczema has cleared as this reduces the risk of flare-ups.
Emollients are moisturising treatments which are used to break the Itch – Scratch Cycle and to maintain the smoothness of the skin. They work by; helping skin retain water, moisturising the skin, easing itching, reducing scaling, softening cracks and protecting the skin. Emollients are therefore a leading symptomatic treatment for eczema, where a patient’s skin has become reddened, dry, itchy and cracked.
The AproDerm® range of emollients are for the management and symptomatic treatment of eczema:
![]() They work by forming a protective layer over the skin surface, trapping in water which then goes into the corneocytes, rehydrating them and causing them to swell again. AproDerm® also penetrates through the upper layers of the stratum corneum filling the gaps between the corneocytes so that they are once again surrounded (mimicking the lipid lamellae) thus restoring the skin barrier so that irritants, pathogens and allergens are kept out whilst keeping in water and other substances. Rehydration of the skin helps relieve the itching, irritation and discomfort associated with eczema.
They work by forming a protective layer over the skin surface, trapping in water which then goes into the corneocytes, rehydrating them and causing them to swell again. AproDerm® also penetrates through the upper layers of the stratum corneum filling the gaps between the corneocytes so that they are once again surrounded (mimicking the lipid lamellae) thus restoring the skin barrier so that irritants, pathogens and allergens are kept out whilst keeping in water and other substances. Rehydration of the skin helps relieve the itching, irritation and discomfort associated with eczema.
![]() AproDerm® Colloidal Oat Cream has a number of additional benefits and mechanisms of action. Formulated with active colloidal oatmeal which is proven to protect and restore the skin’s surface, oatmeal has been used for centuries as a soothing agent to relieve itch and irritation, and has been clinically proven to improve dryness, scaling and roughness. With its direct anti-inflammatory and anti-oxidant activities, colloidal oat restores the epidermal barrier damaged by eczema. AproDerm® Colloidal Oat Cream also has humectant, buffering and cleansing effects.
AproDerm® Colloidal Oat Cream has a number of additional benefits and mechanisms of action. Formulated with active colloidal oatmeal which is proven to protect and restore the skin’s surface, oatmeal has been used for centuries as a soothing agent to relieve itch and irritation, and has been clinically proven to improve dryness, scaling and roughness. With its direct anti-inflammatory and anti-oxidant activities, colloidal oat restores the epidermal barrier damaged by eczema. AproDerm® Colloidal Oat Cream also has humectant, buffering and cleansing effects.
For further information on the AproDerm® Range Click Here

AproDerm® Range
AproDerm® is a range of dermatologically tested, occlusive, leave-on emollients, which are suitable from birth. They are specially formulated (patent pending) with the patient in mind and are free from the potential irritants and sensitisers SLS, parabens, halogens, fragrances and colours
Read More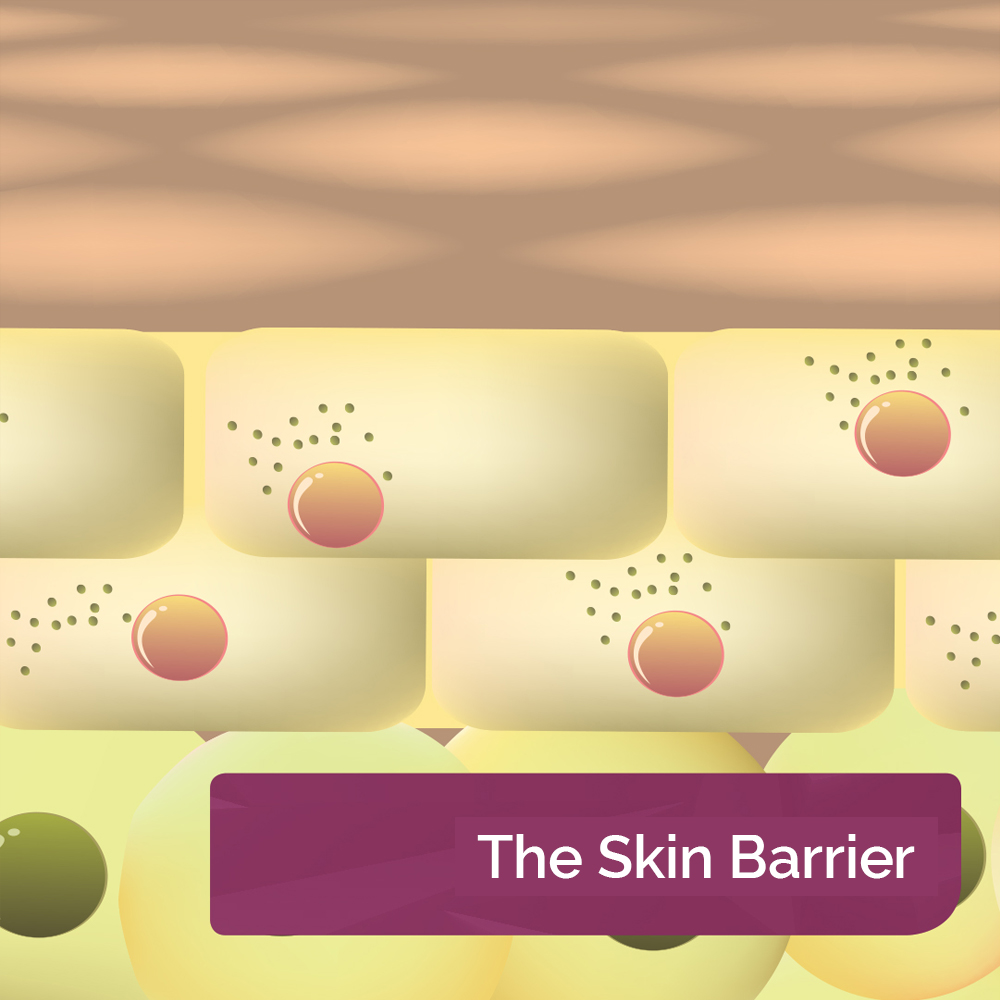
The Skin Barrier
The Stratum Corneum or Skin Barrier is the uppermost layer of the epidermis and its role is to protect against pathogens, allergens and irritants whilst keeping water and other substances in the body
Read More
Psoriasis
Psoriasis affects 1-3% of the UK population and about 80 million worldwide. It is a multi-factorial condition involving genetics, the immune system and environmental triggers
Read More

Dry Skin Conditions
There are a number of factors which can contribute as to why a patient has Xerosis or dry skin. These include the environment, genetics, underlying medical conditions and the side-effects of certain medications
Read More
Why Use AproDerm®?
AproDerm® is free from excipients such as SLS, parabens, halogens, fragrances and colours which can irritate and sensitise skin with eczema sufferers being particularly sensitive to their effects
Read More
Request Samples
Help your patients discover the benefits of AproDerm® – free samples of our emollients and barrier creams are available to all Healthcare Professionals, simply follow the link.
Request Samples